

The adjustment of the training load in rehabilitation exercises is usually done according to factors such as pain (VAS scale), perceived effort (BORG scale), number of repetitions and series, time of evolution of the case, and each patient’s requirements.
However, as we will see in this case, there is a factor that can be crucial and that is usually missed: scapulohumeral movement impairments.
Elevation movement in scapular plane (Scaption) is often introduced in rehabilitation programs when the patient is getting ready to perform movements to reach overhead in open kinetic chain. Sciascia et als. showed that, during this exercise the activation levels were useful for some muscles, such as supraspinatus, infraspinatus and serratus anterior (1)
Specifically, the activation of the serratus anterior muscle increases as the elevation angle gets higher. Furthermore, in both concentric and eccentric phases of the movement, this activation remains higher than 20% MVIC (Maximum Voluntary Isometric Contraction), which is the minimum level of activation to consider an exercise as effective to improve the strength of this muscle (2).
Because the Scaption exercise implies at the same time the activity of rotator cuff and serratus anterior muscles, it could be considered ideal training for shoulder stability through muscle coordination.
One very interesting aspect to consider about this exercise is how muscle activation values change depending on the load.
Castelein et als., from Ghent University( Belgium) compared, in a laboratory study, muscle activation during scaption exercise with and without load in 21 subjects(3).
Results are shown in this graph:
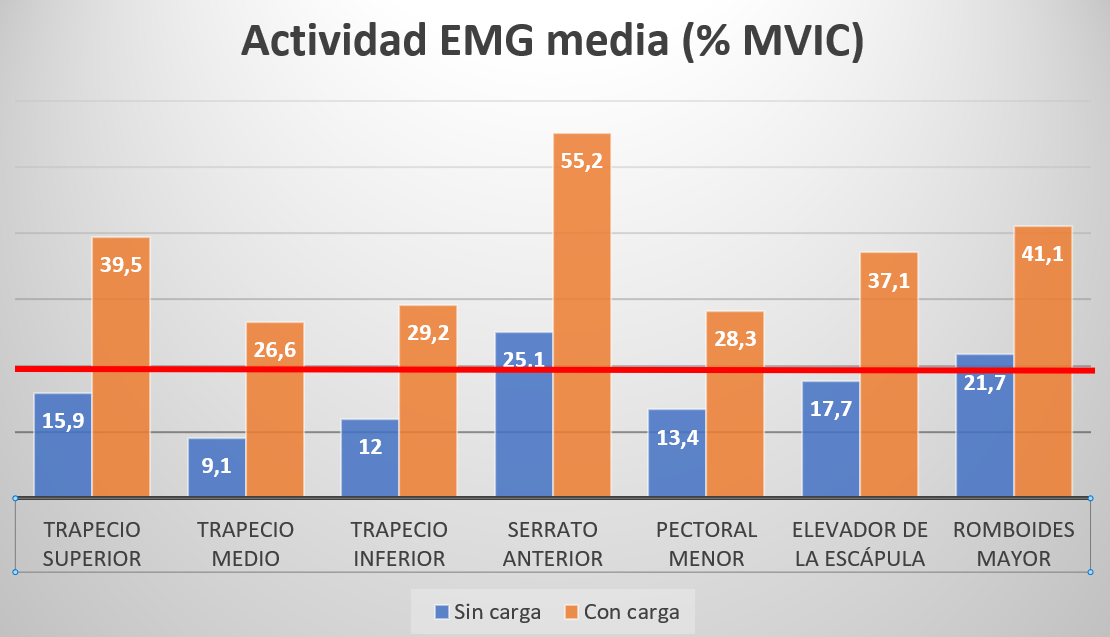
We can see how, as the load increases, serratus anterior activation is doubled. Also, activation of the three parts of the trapezius reaches 20%, which makes this exercise effective to strengthen the trapezius if you load it.However, we can also see the same change with other muscles such as the pectoralis minor, levator of scapula and rhomboid major.
What does this imply in the practical field?
Pectoralis minor, levator of scapula and rhomboid major participate in the downward rotation of the scapula, so their strengthening should be limited in those patients presenting scapular upward rotation deficit. This movement impairment has been observed in patients with shoulder pathology, specifically in subacromial impingement and glenohumeral instability (4,5). In addition, Scapular Assistance Test,in which scapular upward rotation is manually assisted during elevation, has shown that symptoms can be modified in one third of the patients with shoulder pathology and in 48,5% of those who presented scapular dyskinesis (6); this finding suggests the implication of this movement in these patients´ clinical findings.
As a conclusion we can say that before loading scaption exercise, it is important to assess that scapular upward rotation is within normality, to ensure that we do not promote muscular imbalances within scapular rotation.
Linking the scientific findings of these researchers to general practice is the real value for our professional development and enables us to achieve the best results in our treatments.
We will talk all about this and more in our course organized by the Chartered Society of Physiotherapy of the Basque Country, which will take place in Bilbao on the 27-29th of September 2019.
Combining science, exercise and technology is the most effective way to approach shoulder pathology.
- “Electromyographical comparison of four common shoulder exercises in unstable and stable shoulders” SCIASCIA A,KUSCHINSKY N,NITZ AJ,MAIR SD,UHL T. Rehabilitation Research and Practice Volume 2012, Article ID 783824, 11 pages
- “A comparison of serratus anterior muscle activation during a wall slide exercise and other traditional exercises” HARDWICK DH, BEEBE JA, MCDONNELL MK, LANG CE. J Orthop Sports Phys Ther. 2006 Dec; 36(12):903-10.
- “Superficial and deep scapulothoracic muscle electromyographic activity during elevation exercises in the scapular plane” CASTELEIN B, CAGNIE B, PARLEVLIET T, COOLS A. J Orthop Sports Phys Ther. 2016 Mar;46(3):184-93
- “Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability” STRUYF F, NIJS J, BAEYENS JP, MOTTRAM S, MEEUSEN R. Scand J Med Sci Sports. 2011 Jun;21(3):352-8
- “The association of scapular kinematics and glenohumeral joint pathologies” LUDEWIG PM, REYNOLDS JF. J Orthop Sports Phys Ther. 2009 February;39(2):90-104
- “A positive scapular assitance test is equally present in various shoulder disorders but more commonly found among patients with scapular dyskinesis”RABIN A, CHECHIK O, DOLKART O, GOLDSTEIN Y, MAMAN E. Phys Ther Sport. 2018 Nov;34:129-135